
Brief description
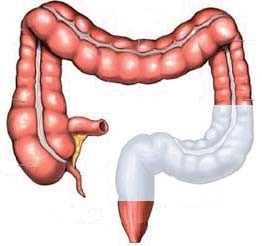
A large bowel resection is an operation to remove all or part of the large bowel or colon because it is diseased or not working properly. The bowel is like a hollow tube. The surgeon will cut out part of the bowel and sew or staple the remaining ends together (an anastomosis). The amount of bowel removed varies, depending on the reason for the operation.
Why is this operation necessary?
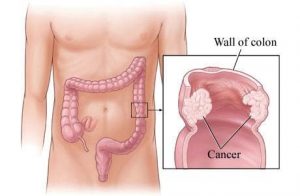
There is a disease in the colon. Common reasons for this operation are cancer, diverticular disease, inflammatory bowel disease, a stricture or narrowing which is causing a blockage.
Are there alternative treatments available?
The colon can also be removed with a laparoscopic procedure, if you and your surgeon are comfortable with this approach. Your surgeon will discuss with you the advantages and disadvantages of the surgical options.
Is it safe to have this operation?
Before you agree to the operation, you should consider the risks that may be involved. Your surgery will be performed by a team of highly qualified and skilled professionals who will take all steps necessary to ensure a safe procedure and a successful result. However there are risks involved with all surgery.
WHAT ARE THE GENERAL RISKS INVOLVED?
These are risks which may occur with any surgical procedure. These complications include the risk of infection, bleeding, pain, wound breakdown, deep vein thrombosis, or complications affecting the heart, lungs or kidneys.
WHAT ARE THE SPECIFIC RISKS INVOLVED?
The main complication is an anastomotic leak which may bleak at the new join. This can take up to a week to declare itself, and you will be closely monitored for this in the early days. This occurs in less than 5-10% of patients. It can be life-threatening, and you may require emergency re-look surgery to wash out infection. It may be necessary to give you a temporary colostomy or bag. Other risks include bowel blockage, a wound infection, ileus which is paralysed bowel causing nausea and vomiting and bleeding. A late complication can be an incisional hernia, especially if there was infection in the wound.
WHAT ARE THE ANAESTHETIC RISKS INVOLVED?
You can discuss the general anaesthetic requirements with your anaesthetist and also the possible complications that may occur.
You should not eat anything solid for at least six hours before your operation. You can usually drink clear liquids until 2 hours before the operation, but discuss this with your surgeon or the nurses, if unsure.
You should take all your regular medication as usual on the day. Your surgeon may want you to stop certain medication such as disprin, warfarin, or other blood thinning medicines before the operation. You may be given high energy drinks in the days preceding your operation or even on the day of the operation.
In some cases your surgeon may give you some preparation to empty your bowels. If you are asked to take this laxative, you will usually experience some abdominal cramps and have your bowels open several times very urgently – so make sure you know where the toilets are. You will be given an instruction sheet for this. In other cases your surgeon may decide that your bowel does not need preparing in this way, or you may be administered an enema in order to empty the last part of the bowel.
You may be given some white stockings to wear during and after the operation. It is also usual for you to be given a small injection in your arm or tummy once a day. Both of these measures help prevent blood clots in your legs. While a stoma or bag is not usually necessary for this procedure, it is sometimes required. For this reason you may see the colorectal nurse specialist, or stomatherapist, preoperatively to have a mark made on your abdomen. This will guide the surgeon where to place the stoma, if needed.
WHAT HAPPENS BEFORE THE OPERATION?
Before surgery, routine tests will be performed, you may be seen by a specialist physician who will also visit you daily after surgery.
Please report to the hospital reception on time for your admission. Please bring along all the documents that may be required such as your medical aid card, ID and contact details. If you are not a member of a medical aid you will be required to pay a deposit or to sign an indemnity form. As far as possible we will try to advise you about hospital costs before your admission.
When you arrive in the ward, you will be welcomed by the nurses or the receptionist and will have your details checked. Some basic tests will be done such as pulse, temperature, blood pressure and urine examination. You will be asked to hand in any medicines or drugs you may be taking, so that your drug treatment in hospital will be correct. Please tell the nurses of any allergies to drugs or dressings. The surgeon will have explained the operation and you may be asked to sign another consent for the operation. If you are not clear about any part of the operation, ask for more details from the surgeon or from the nurses.
The operation area may need to be shaved to remove excess hair. This may be done in the ward or in the theatre after you are asleep. You may be issued with compression stockings that will help prevent blood clots in your legs. If you are having a general anaesthetic, the anaesthetist who will be giving your anaesthetic will interview and examine you and he may put up a drip or prescribe some medication to help you relax.
You will be taken on a bed to the operating suite by the staff. You will be wearing a cotton gown with disposable hospital underwear, wedding rings will be fastened with tape and removable dentures will be left on the ward. There will be several checks on your details on the way to the operating theatre where your anaesthetic will begin.
HOW LONG DOES THE OPERATION TAKE?
2-5 hours
WHAT HAPPENS WHEN I WAKE UP?
After the operation you will be transferred back to the ward/ICU/ HCU. Although you will be conscious a minute or two after the operation ends, you are unlikely to remember anything until you are back in your bed. On your return to the ward you may feel quite sleepy but will be aware of the drips and drains that are present. You will have a dressing over the surgical wound on your abdomen. The nurse will replace the dressing as necessary. A drip will be in your arm or neck in order to maintain your hydration and give you some energy. A catheter is placed into your bladder in order to drain urine. You may have a catheter in your back for an infusion of pain medication. This is called an epidural, and your anaesthetist will have explained this to you.
You may find that you have a sore throat or husky voice for a few days after the operation. This is because the tube used to help you breathe during the operation often bruises the delicate lining in your throat and vocal chords. Gargles may help ease any soreness, which should go within a few days.
You can have a bath or shower as soon as you feel able, often within days of the operation. You are bound to feel a little wobbly at first, so ask for help if you need it, or at least let your nurse know where you are going, and use the nurse call button if you need to.
At first you will be helped to do most things by the nurses. The amount of nursing care you receive generally decreases as you be- come increasingly independent. The catheter will usually stay in your bladder for a few days until you are able to get to the toilet yourself. Your stitches or clips will be taken out after about 10 to 14 days. I They may be disolvable in which case they will not need to be removed. It can be difficult to sleep well in hospital due to the change of surroundings, the need for observation and the tubes attached to you. A sleeping pill is usually offered. Some patients also experience strange dreams in the first few nights after the anaesthetic. Elderly patients may suffer some disorientation and confusion. You should find that your sleep improves after the first week or once you have returned home. In the first few days you will feel tired and may want to request that only close family and friends visit, and to keep visits quite short.
WILL I HAVE PAIN?
We will aim for you to be as pain free as possible. Some discomfort is to be expected, particularly when getting in and out of the bed or chair.
Painkillers will usually be given continuously via the epidural catheter or a pump during the first few days after your operation. Please discuss with your nurse if you feel that your pain is not well controlled and remember that over use of your pain medication may prolong your hospital stay due to may factors.
HOW SOON AFTER THE OPERATION CAN I EAT?
Surgeons vary as to when they let you start eating. Once you have passed wind, which can take a few days, you will first be allowed small amounts of fluid, gradually building up to being able to drink as much as you like. Once you are drinking normally you will usually be encouraged to start eating a light diet.
HOW SOON AFTER THE OPERATION CAN I GET OUT OF BED?
We will usually get you up into a chair the first day after your operation, for some people the same day of the operation. This is to help get your circulation moving. The stockings on your legs may feel hot, but they are very important to help to prevent blood clots. While you are in bed it is a good idea to point your toes up and down and to gently exercise your legs. You should sit up rather than lying flat and take six deep breaths an hour, expanding your chest as fully as possible. The physiotherapist will probably visit you and show you some chest exercises and make you cough any phlegm up off your chest. You can cuddle a towel or small pillow across your abdomen for support when coughing. If deep breathing is painful you should discuss pain relief with your nurse and try to get as comfortable as possible before the physiotherapist visits.
HOW LONG WILL I STAY IN THE HOSPITAL?
5-10 days, provided there are no complications
WHAT HAPPENS WHEN I AM DISCHARGED FROM THE WARD?
Your surgeon will determine when you are ready to go home. You will be given some medication for pain and you may also need to take antibiotics for a few days after you go home. You will be given instructions on the dressings and how to care for the wound. You will also get an appointment for your follow-up in the surgeon’s rooms. You should ask for a sick certificate if you need this for your employer.
WHAT SHOULD I BE AWARE OF WHEN I GET HOME?
Initially your bowel actions are very likely to be a bit unpredictable. It can take several months for this to settle and for you to develop a predictable pattern. Your bowel function is unlikely to be exactly the same as it was before your operation, so your expectation of what is “normal” for you may need to be adjusted. If a large portion of the colon has been removed then your stool may always be looser, as less water will be absorbed from it. It takes time for the bowel that remains to compensate for that which has been removed, and it may never completely do so.
If diarrhea becomes a persistent problem, discuss this with your doctor. There are medicines which can thicken the stool and some people do need to take medicine on a permanent basis.
It would also be unwise to go swimming until the area has completely healed. You can resume sexual activity as soon as this feels comfortable.
Having an operation can be a stressful experience, physically and emotionally. In the first weeks at home you may have some days when you feel quite low and this is normal. Some people find that it can take some months to adjust emotionally to the surgery. When you first go home you are likely to feel tired and vulnerable for a while. Things will get better. Some people report that it takes them 3 to 6 months to feel completely back to their normal selves, others recover much more quickly. It is common to feel a bit low in the first weeks and to become frustrated that you cannot do everything that you would like to do. Be patient! Restrict visitors, rest plenty, don’t push yourself, take a gentle short walk if you feel like it. Eat simply, in smaller more frequent quantities. Keep an eye on your wound for any late inflammation or infection, and report it promptly.
HOW SOON CAN I START EXERCISE?
The time taken to get back to normal activities varies a lot for different people. Do as much as you feel comfortable doing. If you need to take painkillers these may make you drowsy, so you should avoid driving or operating machinery. If lifting causes you discomfort you should avoid it. Expect roughly 4-6 weeks before intense physical exercise can be performed
HOW SOON CAN I DRIVE A CAR?
Discuss this with the surgeon at your post-op visit. You should not drive until you feel confident that you could manage an emergency stop.
HOW LONG WILL I BE OFF WORK?
Most people need about four to six weeks off work, but this will depend a little on what you do and it is important for you to pay attention to your body, balancing doing as much as you feel able to with exercising enough to regain your strength and confidence .