
Brief description
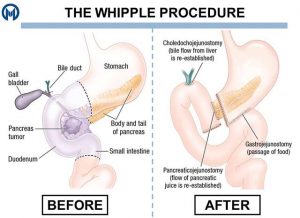
This is a major operation to remove the head of the pancreas. A large incision (cut) is made right across the upper abdomen (tummy) below the ribs on both sides. The abdomen is checked to make sure there are no signs of tumour spread beyond the pancreas. There are variations in how the operation is performed and the stomach may be fully preserved or only a small portion removed. The head half of the pancreas is then cut out, leaving behind the tail half of the pancreas. The head of the pancreas is closely attached to the duodenum (first part of the small bowel after the stomach), and the bile duct coming from the liver runs through the pancreas. The duodenum and bile duct are thus also removed. The stomach, top end of the bile duct, and tail end of the pancreas are then each joined separately to the small intestine. If it is discovered at surgery that the tumour has spread further than was seen on the scans, and that removal of the pancreas will not remove all the tumour, then a bypass procedure may be performed. Here the bile duct and stomach are stitched to the small bowel, in order to relieve blockages, but the pancreas is not removed.
WHY IS THIS OPERATION NECESSARY?
A Whipple’s resection is performed with the intention of obtaining complete removal of a suspected tumour, situated in the head of the pancreas. The operation is only of potential benefit if the tumour can be completely removed. Even when the operation has been successful, the cancer often still recurs thus cure is not guaranteed. Chemotherapy is often prescribed after successful surgery.
Are there alternative treatments available?
This is the only treatment performed with the intention of cure. Other less invasive treatments such as placement of stents (tubes) in the bile duct serve to relieve symptoms such as jaundice, but do not result in cure. Chemotherapy In cases where the tumour is felt to be unresectable based on the scans performed. Initial chemotherapy (and sometimes radiotherapy) may be offered in order to attempt to shrink the tumour and allow for later successful resection. This is referred to as neoadjuvant therapy.or radiotherapy are not curative.
Is it safe to have this operation?
Before you agree to the operation, you should consider the risks that may be involved. Your surgery will be performed by a team of highly qualified and skilled professionals who will take all steps necessary to ensure a safe procedure and a successful result. However there are risks involved with all surgery even if these risks may be small.
WHAT ARE THE GENERAL RISKS INVOLVED?
There are risks for developing complications which are general and which may occur with any surgical procedure. These complications include the risk of infection, bleeding, pain, wound breakdown, deep vein thrombosis, or complications affecting the heart, lungs or kidneys. A blood transfusion may be required.
WHAT ARE THE SPECIFIC RISKS INVOLVED?
A complication of some description occurs in around 40% of patients. These complications are usually minor, and although they result in a prolonged hospital stay, usually resolve. The most significant complications are related to leaks from any of the three major joins, particularly leaks from the join between the pancreas and the intestine. In up to 5% of cases complications can be more serious, and result in death. In the long term having a reduced amount of pancreas can cause you to become diabetic and require insulin. You can also develop impaired digestion of food and resultant fatty stools (steatorrhoea). This is treated with enzyme replacement capsules. One of these problems occurs in about a third of people in the long term.
WHAT ARE THE ANAESTHETIC RISKS INVOLVED?
You can discuss the type of anaesthetic you will have with your anaesthetist and also the possible complications that may occur.
WHAT SHOULD I DO BEFORE THE OPERATION?
In the weeks prior to the operation you will be seen by a physician and a dietician. On the day of the operation you should not eat or drink anything for at least six hours before your operation. However, you should take all your regular medication as usual on the day. You should stop certain medication such as disprin, warfarin, or other blood thinning medicines a week before the operation. You will be instructed to take a special drink 2 hours before surgery.
WHAT HAPPENS BEFORE THE OPERATION?
Please report to the hospital reception on time for your admission. This will usually be on the day prior to the operation. Please bring along all the documents that may be required such as your medical aid card, ID and contact details. If you are not a member of a medical aid you will be required to pay a deposit or to sign an indemnity form. As far as possible we will try to advise you about hospital costs before your admission. It may be best to complete some of the documentation beforehand at the hospital pre-admission clinic to save time on the day of your admission.
When you arrive in the ward, you will be welcomed by the nurses or the receptionist and will have your details checked. Some basic tests will be done such as pulse, temperature, blood pressure and urine examination. You will be asked to hand in any medicines or drugs you may be taking, so that your drug treatment in hospital will be correct. Please tell the nurses of any allergies to drugs or dressings. The surgeon will have explained the operation and you will be asked to sign your consent for the operation. If you are not clear about any part of the operation, ask for more details from the surgeon or from the nurses.
In an adult the operation area may need to be shaved to remove excess hair. You may be issued with compression stockings that will help prevent blood clots in your legs. The anaesthetist who will be giving your anaesthetic will interview and examine you and he may put up a drip or prescribe some medication to help you relax.
You will be taken on a trolley to the operating suite by the staff. You will be wearing a cotton gown. Wedding rings will be fastened with tape and removable dentures will be left on the ward. There will be several checks on your details on the way to the operating theatre where your anaesthetic will begin.
HOW LONG DOES THE OPERATION TAKE?
This is a very long and complex procedure, and can be quite variable in length. It is usually at least 6-7 hours in duration.
WHAT HAPPENS WHEN I WAKE UP?
After the operation is completed you will be transferred to ICU. The anaesthetist may choose to keep you on a ventilator after the surgery, in which case you will only wake up fully the following day. Otherwise you will wake up when in the ICU. You will have a drip in your neck (CVP line)and one in your wrist (arterial line), a tube in your nose (Naso-gastric tube), and three tubes coming out of your belly (one used for feeding directly into the small intestine, and two to drain out any fluid that may accumulate).
WILL I HAVE PAIN?
Some pain may be present. You will have an epidural catheter in your back placed prior to surgery by the anaesthetist, which will help to control the pain for 3 days while you are in the ICU. The level of pain should always be reasonably controlled, although some degree of pain is usually unavoidable. Ask the nursing staff for medication if you have pain.
HOW SOON AFTER THE OPERATION CAN I EAT?
You can have sips of water as soon as you are awake. Feeds will be introduced gradually over several days.
HOW SOON AFTER THE OPERATION CAN I GET OUT OF BED?
You will be encouraged to mobilize as much as possible, but initially this will be limited with the epidural in place. The level of exercise can be built up steadily in the ward.
HOW LONG WILL I STAY IN THE HOSPITAL?
If everything goes smoothly the usual stay is 12-14 days. However if there are any complications such as a leak from the pancreas the stay may be longer.
WHAT HAPPENS WHEN I AM DISCHARGED FROM THE WARD?
Your surgeon will determine when you are ready to go home. You will be given some medication for pain. You will be given instructions on the dressings and how to care for the wound. You will also get an appointment for your follow-up in the surgeon’s rooms. You should ask for a sick certificate if you need this for your employer.
WHAT SHOULD I BE AWARE OF WHEN I GET HOME?
Any high fevers, or persistent vomiting should be reported promptly.
HOW SOON CAN I START EXERCISE?
You can start walking straight away, but it is likely to be several weeks before you are back to full strength and activity.
HOW SOON CAN I DRIVE A CAR?
This depends on your recovery, but usually you should avoid driving for about two weeks after discharge from hospital.
HOW LONG WILL I BE OFF WORK?
You should expect to be off work for at least a month 4 to 6 weeks depending on the recovery and whether complications occurred.
An overview of the Whipple’s procedure
What us the Whipple’s procedure?