
Brief description
The Nissen fundoplication operation is performed to relieve gastro- oesophageal reflux (GORD). Reflux may be associated with an hiatus hernia. A hiatus simply means a gap/opening. A hernia is a bulge or a weakness. In this case, the stomach bulges through a hiatus up into your chest. Sometimes the stomach gets stuck within the chest. Your surgeon will
discuss the procedure with you in detail and will answer any questions you may have before the operation.
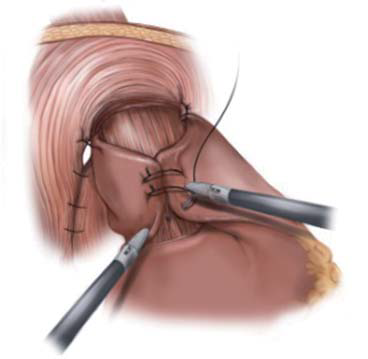
 The aim of the operation is to bring the stomach down from the chest and to stop the acid reflux. A telescope with an attached miniature TV camera (laparoscope) is inserted through a small (1 cm) incision above the belly button (umbilicus). Four other similar incisions are made to insert the necessary instruments for the operation. The herniated stomach and the lowest part of the oesophagus are returned to their normal positions i.e. below the diaphragm. Part of the stomach (fundus) is wrapped around the oesophagus to re-create a valve. The hiatus in the diaphragm is narrowed with stitches. The instruments are withdrawn and the incisions are closed. In a small number of patients (approx. 5%) it may not be possible to operate via the laparoscope due to adhesions from previous operations, bleeding obscuring vision, awkward fatty tissue or other technical problems. It will then be necessary to revert to the standard (open) operation.
The aim of the operation is to bring the stomach down from the chest and to stop the acid reflux. A telescope with an attached miniature TV camera (laparoscope) is inserted through a small (1 cm) incision above the belly button (umbilicus). Four other similar incisions are made to insert the necessary instruments for the operation. The herniated stomach and the lowest part of the oesophagus are returned to their normal positions i.e. below the diaphragm. Part of the stomach (fundus) is wrapped around the oesophagus to re-create a valve. The hiatus in the diaphragm is narrowed with stitches. The instruments are withdrawn and the incisions are closed. In a small number of patients (approx. 5%) it may not be possible to operate via the laparoscope due to adhesions from previous operations, bleeding obscuring vision, awkward fatty tissue or other technical problems. It will then be necessary to revert to the standard (open) operation.
Why is this operation necessary?
Majority of patients are well controlled on medication and only a small subgroup will require surgery. Indications include, volume reflux, symptomatic hernia, side effects from medication or need to avoid life long medical treatment.
Are there alternative treatments available?
Most patients will be well controlled on medication.
Is it safe to have this operation?
Your surgery will be performed by a team of highly qualified and skilled professionals who will take all steps necessary to ensure a safe procedure and a successful result. However there are risks involved with all surgery even if these risks may be small. Before you agree to the operation, you should consider the risks that may be involved.
WHAT ARE THE GENERAL RISKS INVOLVED?
There are risks for developing complications which are general and which may occur with any surgical procedure. These complications include the risk of infection, bleeding, pain, wound breakdown, deep vein thrombosis, or complications affecting the heart, lungs or kidneys.
WHAT ARE THE SPECIFIC RISKS INVOLVED?
Most patients have a good result from the fundoplication operation without any complications. However the main complication,(less than 2%) which can be serious, is injury to the oesophagus. There is also risk of injury to the stomach, colon, spleen and liver. These will usually be recognized at the time of surgery and may require an open operation to repair it. On occasion patients will present a few days later and then require a second operation. A small number of patients who have the laparoscopic fundoplication may
develop problems either due to the wrap being too tight or the wrap slipping into the chest. These can sometimes be corrected by early laparoscopic re-operation lengthening the recovery time by a few days. To detect complications after laparoscopic fundoplication and early enough for laparoscopic repair, a barium x-ray will sometimes be performed in the first 1-3 days after operation, which allows the position and construction of the wrap to be checked. It is quite normal for there to be some difficulty in the passage of food through the oesophagus into the stomach after this type of surgery. This is generally due to the swelling and bruising at the site of the operation, and while this will gradually resolve, it may take 3-6 months for swallowing to return completely to normal. A small number of patients this can be more severe and it may be necessary to dilate (stretch) the lower end of the oesophagus. This is usually done in our rooms with a flexible scope. Other risks are delayed return of bowel function, wound infection, deep vein thrombosis, pulmonary emboli, atelectasis and pneumonia. Late complications may occur such as a suture granuloma or a hernia at the site of the wound.
WHAT ARE THE ANAESTHETIC RISKS INVOLVED?
You can discuss the type of anaesthetic you will have with your anaesthetist and also the possible complications that may occur.
WHAT SHOULD I DO BEFORE THE OPERATION?
You should not eat or drink anything for at least six hours before your operation. However, you should take all your regular medication as usual on the day. Your surgeon may want you to stop certain medication such as disprin, warfarin, or other blood thinning medicines before the operation.
WHAT HAPPENS BEFORE THE OPERATION?
Please report to the hospital reception on time for your admission. Please bring along all the documents that may be required such as your medical aid card, id and contact details. If you are not a member of a medical aid you will be required to pay a deposit or to sign an indemnity form. As far as possible we will try to advise you about hospital costs before your admission. It may be best to complete some of the documentation beforehand at the hospital pre-admission clinic to save time on the day of your admission. When you arrive in the ward, you will be welcomed by the nurses or the receptionist and will have your details checked. Some basic tests will be done such as pulse, temperature, blood pressure and urine examination. You will be asked to hand in any medicines or drugs you may be taking, so that your drug treatment in hospital will be correct. Please tell the nurses of any allergies to drugs or dressings. The surgeon will have explained the operation and you will be asked to sign your consent for the operation. If you are not clear about any part of the operation, ask for more details from the surgeon or from the nurses. In an adult the operation area may need to be shaved to remove excess hair. You may be issued with compression stockings that will help prevent blood clots in your legs. If you are having a general anaesthetic, the anaesthetist who will be giving your anaesthetic will interview and examine you and he may put up a drip or prescribe some medication to help you relax. You will be taken on a trolley to the operating suite by the staff. You will be wearing a cotton gown. Wedding rings will be fastened with tape and removable dentures will be left on the ward. There will be several checks on your details on the way to the operating theatre where your anaesthetic will begin.
HOW LONG DOES THE OPERATION TAKE?
Usually about 90 minutes.
WHAT HAPPENS WHEN I WAKE UP?
After the operation is completed you will be transferred back to the ward. (Although you will be conscious a minute or two after the operation ends, you are unlikely to remember anything until you are back in your bed on the ward. You will have an oxygen mask and a drip (intravenous) line.
WILL I HAVE PAIN?
Some pain may be present, but this should be controlled to a level of mild discomfort with the painkillers that are prescribed. Ask the nursing staff for medication if you have pain.
HOW SOON AFTER THE OPERATION CAN I EAT?
You will be allowed water, tea or juice in small amounts immediately after the operation, but can only start eating food again the following day.
HOW SOON AFTER THE OPERATION CAN I GET OUT OF BED?
You should be able to walk a short distance very soon after waking up, but ask the nursing staff for assistance if you feel dizzy. You should be able to walk without too much discomfort by the next day and will be encouraged to mobilize as much as possible.
HOW LONG WILL I STAY IN THE HOSPITAL?
Usually 3 days.
WHAT HAPPENS WHEN I AM DISCHARGED FROM THE WARD?
Your surgeon will determine when you are ready to go home. You will be given some medication for pain and possibly injections for deep vein thrombosis prophylaxis. You will be given instructions on the dressings and how to care for the wound. You will also get an appointment for your followup visit in the surgeon’s rooms. You should ask for a sick certificate if you need this for your employer.
WHAT SHOULD I BE AWARE OF WHEN I GET HOME?
You will have a variable amount of difficulty in swallowing, this is common. The key is small frequent meals (every 2 – 3 hours). Avoid bread and red meat in the first week. Should something get stuck a carbonated drink often help.
HOW SOON CAN I START EXERCISE?
You can perform routine activities as soon as you get home including walking or climbing stairs. Normal exercise after 2-3 three weeks. This is best discussed at your first post–operative visit.
HOW SOON CAN I DRIVE A CAR?
7-10 days.
HOW LONG WILL I BE OFF WORK?
Usually between 10-14 days