
Brief description
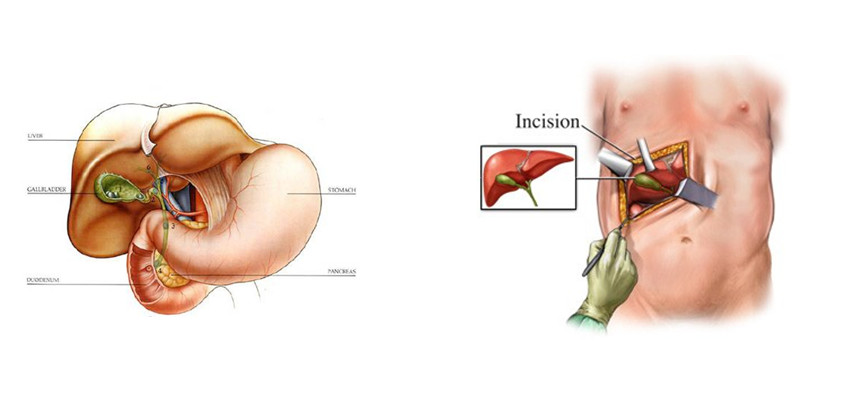
An incision (cut) is made across the upper abdomen (tummy) below the ribs on both sides. The common bile duct (CBD – the main tube carrying bile from the liver to the intestine) is then opened up. Any gallstones within the duct causing a blockage can then be removed. A small camera (choledochoscope) is then passed up the duct into the liver to remove any stones stuck higher up. The gallbladder is removed as part of the same opera- tion. The CBD is then stitched closed. Sometimes the small intestine is brought up and stitched directly to the CBD to bypass any blockage or narrowing lower down the CBD, allowing bile to continue to enter the bowel. This operation may also be performed using minimally invasive laparoscopic surgery by surgeons experienced with this technique. The benefit would be smaller incisions with less postoperative pain and a quicker recovery from surgery.
Why is this operation necessary?
The operation is performed to relieve blockage of the CBD. It is usually performed for blockage of the CBD by gallstones that have worked their way into the CBD from the gallbladder. In most cases previous attempts will have been made to remove the stones by a less invasive scope procedure called ERCP. If the ERCP has failed to remove the stones completely then an open CBD exploration is required. This operation may also be performed for obstruction to the bile duct from scarring or tumours. In these cases, removal of the bile duct may be necessary and a reconstruction of the bile drainage is performed.
Are there alternative treatments available?
The alternative procedure of ERCP (endoscopic retro- grade cholangio-pancreatography) is usually attempted prior to an operation. However if the ERCP is unsuccess-ful then the open operation is required. Breaking up the stones by sound waves,referred to as extracorporeal shock-wave lithotrypsy (ESWL), or laser may be an effective treatment combined with ERCP to break up large stones. If successful, open surgery may not be required.
Is it safe to have this operation?
Before you agree to the operation, you should consider the risks that may be involved. Your surgery will be per- formed by a team of highly qualified and skilled profes- sionals who will take all steps necessary to ensure a safe procedure and a successful result. However there are risks involved with all surgery even if these risks may be small.
WHAT ARE THE GENERAL RISKS INVOLVED?
There are risks for developing complications which are general and which may occur with any surgical proce- dure. These complications include the risk of infection, bleeding, pain, wound breakdown, deep vein thrombosis, or complications affecting the heart, lungs or kidneys.
WHAT ARE THE SPECIFIC RISKS INVOLVED?
The major risk is leakage of bile from the CBD after it has been stitched closed, or stitched directly to the small bowel. Leakage of bile can lead to significant infection within the abdomen if this bile is not drained out.
The longer term risk is if a narrowing of the CBD occurs in the area where it is stitched closed. This may even occur several years later.
WHAT ARE THE ANAESTHETIC RISKS INVOLVED?
You can discuss the type of anaesthetic you will have with your anaesthetist and also the possible complica- tions that may occur.
WHAT SHOULD I DO BEFORE THE OPERATION?
You should not eat or drink anything for at least six hours before your operation. However, you should take all your regular medication as usual on the day. You should stop certain medication such as disprin, warfarin, or other blood thinning medicines before the operation.
WHAT HAPPENS BEFORE THE OPERATION?
Please report to the hospital reception on time for your admission. Please bring along all the documents that may be required such as your medical aid card, ID and con- tact details. If you are not a member of a medical aid you will be required to pay a deposit or to sign an indemnity form. As far as possible we will try to advise you about hospital costs before your admission.
It may be best to complete some of the documentation beforehand at the hospital preadmission clinic to save time on the day of your admission.
When you arrive in the ward, you will be welcomed by the nurses or the receptionist and will have your details checked. Some basic tests will be done such as pulse, temperature, blood pressure and urine examination. You will be asked to hand in any medicines or drugs you may be taking, so that your drug treatment in hospital will be correct.
Please tell the nurses of any allergies to drugs or dressings. The surgeon will have explained the operation and you will be asked to sign your consent for the operation. If you are not clear about any part of the operation, ask for more details from the surgeon or from the nurses.
In an adult the operation area may need to be shaved to remove excess hair. You may be issued with compression stockings that will help prevent blood clots in your legs.
If you are having a general anaesthetic, the anaesthet- ist who will be giving your anaesthetic will interview and examine you and he may put up a drip or prescribe some medication to help you relax.
You will be taken on a trolley to the operating suite by the staff. You will be wearing a cotton gown. Wedding rings will be fastened with tape and removable dentures will be left on the ward. There will be several checks on your details on the way to the operating theatre where your anaesthetic will begin.
HOW LONG DOES THE OPERATION TAKE?
Around 3 hours
WHAT HAPPENS WHEN I WAKE UP?
After the operation is completed you will be transferred to High Care. Although you will be conscious a minute or two after the operation ends, you are unlikely to remember anything until you are in High Care. You will have an epidural catheter placed into your back by the anaesthetist at the start of the operation. This will stay in place after the op to help control pain. You may also have a drip in the neck (CVP line) and a tube in the nose (Naso-gastric tube). You will also have a urinary catheter. You will have a small drain (tube) coming out of the tummy.
WILL I HAVE PAIN?
Some pain is unavoidable with such a big incision, but this should be controlled to a level of mild discomfort with the epidural in place and the painkillers that are prescribed. Ask the nursing staff for medication if you have pain.
HOW SOON AFTER THE OPERATION CAN I EAT?
You can have sips of water as soon as you wake up. Thereafter you will be progressively allowed to have more fluids and ultimately food over the next couple of days.
HOW SOON AFTER THE OPERATION CAN I GET OUT OF BED?
Your ability to climb out of bed will be limited initially by the epidural. However once you return to the ward you will be encouraged to mobilize as much as possible.
HOW LONG WILL I STAY IN THE HOSPITAL?
Usually 7-10 days
WHAT HAPPENS WHEN I AM DISCHARGED FROM THE WARD?
Your surgeon will determine when you are ready to go home. You will be given some medication for pain. You will be given instructions on the dressings and how to care for the wound. You will also get an appointment for your follow-up in the surgeon’s rooms. You should ask for a sick certificate if you need this for your employer.
WHAT SHOULD I BE AWARE OF WHEN I GET HOME?
You should report any high fevers, prolonged vomiting, or jaundice (yellow discolouration of the eyes or skin).
HOW SOON CAN I START EXERCISE?
You can resume walking immediately, but it will be a few weeks before you are able to resume your pre-operative level of activity.
HOW SOON CAN I DRIVE A CAR?
Usually about 2-3 weeks after discharge from hospital.
HOW LONG WILL I BE OFF WORK?
3-4 weeks in total